1. Introduction
Antibiotics represent one of the most significant medical advances of the 20th century, transforming once-deadly infections into treatable conditions. These remarkable compounds target specific bacterial structures or processes while minimizing damage to human cells. However, the rise of antimicrobial resistance threatens to undermine their effectiveness, creating an urgent global health challenge.

2. Types of Antibiotics and Their Targets
Antibiotics can be classified based on their molecular targets within bacterial cells. Each class exploits differences between bacterial and human cellular machinery to achieve selective toxicity.
Cell Wall Synthesis Inhibitors
The bacterial cell wall, composed primarily of peptidoglycan, provides structural integrity and protection. Human cells lack this structure, making it an ideal antibiotic target.
Beta-lactams (penicillins, cephalosporins, carbapenems)
- These antibiotics contain a beta-lactam ring that binds to penicillin-binding proteins (PBPs), enzymes essential for peptidoglycan cross-linking
- By inhibiting transpeptidase activity, beta-lactams prevent proper cell wall formation
- As bacterial cells grow and divide without proper wall synthesis, they become structurally unstable and eventually rupture
Glycopeptides (vancomycin, teicoplanin)
- Form complexes with D-alanyl-D-alanine terminals of peptidoglycan precursors
- This binding physically blocks transpeptidases and transglycosylases from accessing their substrates
- The resulting inhibition of cell wall synthesis leads to compromised structural integrity and cell death
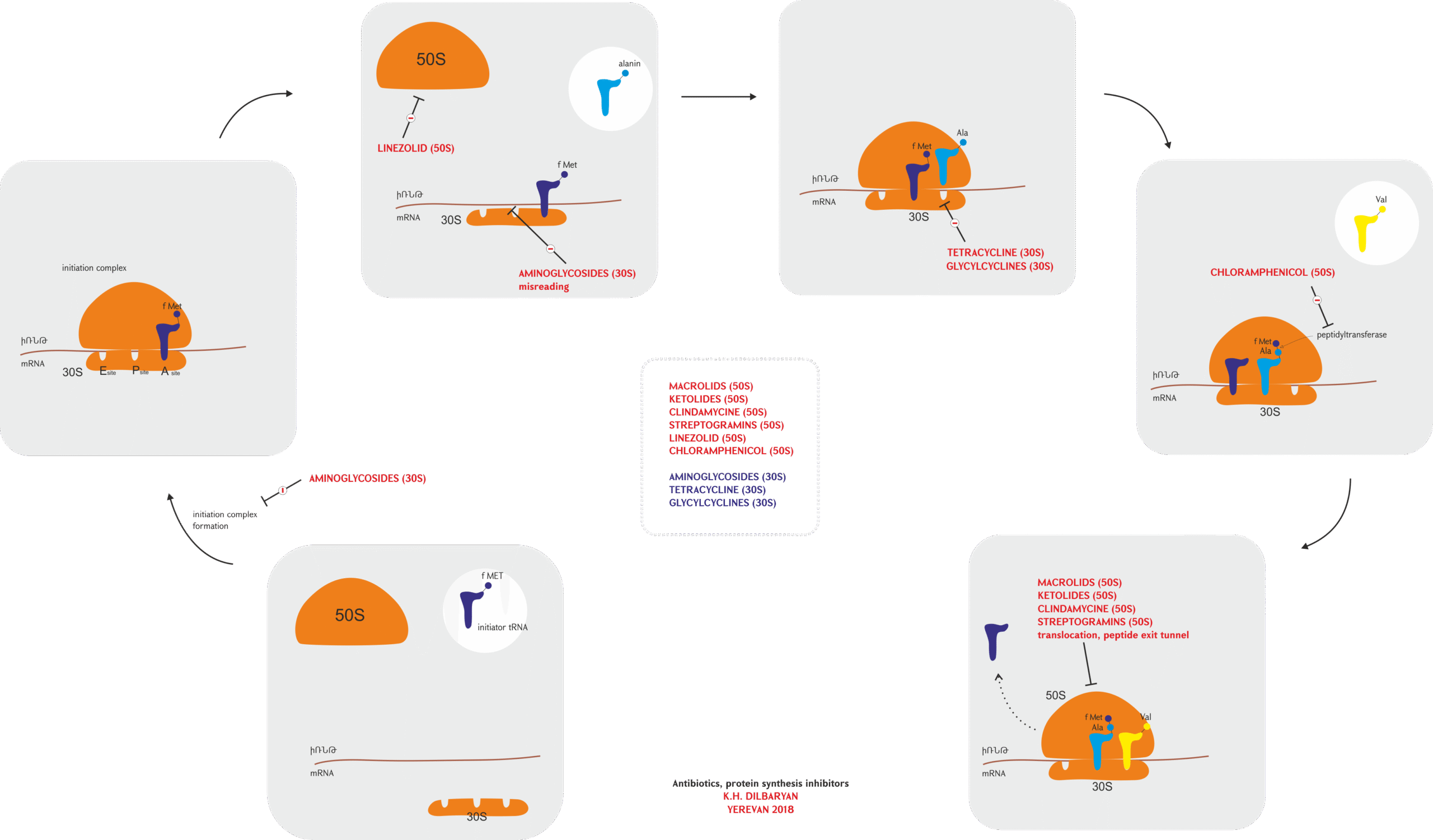
Protein Synthesis Inhibitors
Bacterial ribosomes (70S) differ structurally from human ribosomes (80S), allowing antibiotics to selectively disrupt bacterial protein synthesis.
| Antibiotic Class | Examples | Target | Mechanism |
|---|---|---|---|
| Aminoglycosides | Gentamicin, Streptomycin | 30S ribosomal subunit | Bind to 16S rRNA, causing misreading of mRNA and production of defective proteins |
| Tetracyclines | Doxycycline, Minocycline | 30S ribosomal subunit | Block the attachment of aminoacyl-tRNA to the ribosomal acceptor site |
| Macrolides | Erythromycin, Azithromycin | 50S ribosomal subunit | Bind to 23S rRNA, blocking the peptide exit tunnel and halting peptide chain elongation |
| Chloramphenicol | Chloramphenicol | 50S ribosomal subunit | Inhibits peptidyl transferase activity, preventing peptide bond formation |
| Lincosamides | Clindamycin | 50S ribosomal subunit | Interfere with peptide chain initiation and elongation |
| Oxazolidinones | Linezolid | 50S ribosomal subunit | Prevent formation of the 70S initiation complex |
DNA and RNA Synthesis Inhibitors
These antibiotics interfere with nucleic acid replication, transcription, or repair pathways.
Fluoroquinolones (ciprofloxacin, levofloxacin)
- Target bacterial DNA gyrase and topoisomerase IV
- These enzymes normally introduce negative supercoils in DNA and separate daughter chromosomes after replication
- Fluoroquinolones stabilize the enzyme-DNA complex after strand breakage but before resealing
- The resulting DNA fragmentation triggers SOS response systems and eventually leads to cell death
Rifamycins (rifampin)
- Bind to the β-subunit of bacterial RNA polymerase
- This binding blocks the RNA polymerase channel, preventing RNA chain initiation
- By inhibiting transcription, rifamycins rapidly halt bacterial protein synthesis
Cell Membrane Disruptors
Polymyxins (colistin, polymyxin B)
- Cationic peptides that interact with the lipopolysaccharide (LPS) component of gram-negative bacterial outer membranes
- Displace stabilizing Ca²⁺ and Mg²⁺ ions from the LPS
- This destabilization creates gaps in the membrane, increasing permeability
- The resulting leakage of cellular contents leads to bacterial death
Daptomycin
- Binds to bacterial cell membranes in a calcium-dependent manner
- Forms aggregates that create ion channels or pores
- Causes rapid membrane depolarization and potassium efflux
- The loss of membrane potential leads to inhibition of protein, DNA, and RNA synthesis
Metabolic Pathway Inhibitors
Sulfonamides (sulfamethoxazole) and Trimethoprim
- Target different steps in the bacterial folate synthesis pathway
- Folate is essential for nucleic acid synthesis and cellular replication
- Sulfonamides are structural analogs of para-aminobenzoic acid (PABA) and competitively inhibit dihydropteroate synthase
- Trimethoprim inhibits dihydrofolate reductase
- When used together, these drugs provide synergistic blockade of the folate pathway
3. Mechanisms of Antibiotic Resistance
Bacteria have evolved numerous mechanisms to survive antibiotic exposure. These resistance mechanisms can be intrinsic (inherent to the bacterial species) or acquired through genetic changes.
Enzymatic Inactivation
Bacteria produce enzymes that modify or degrade antibiotics, rendering them ineffective.
| Enzyme Family | Target Antibiotics | Mechanism |
|---|---|---|
| Beta-lactamases | Penicillins, Cephalosporins | Hydrolyze the beta-lactam ring, destroying antibiotic activity |
| Aminoglycoside-modifying enzymes | Aminoglycosides | Add acetyl, phosphate, or adenyl groups to the antibiotic, preventing ribosome binding |
| Chloramphenicol acetyltransferases | Chloramphenicol | Acetylate hydroxyl groups, preventing binding to the ribosome |
| Erythromycin esterases | Macrolides | Hydrolyze the macrolide lactone ring |
Beta-lactamases represent one of the most clinically significant resistance mechanisms. These enzymes have diversified into multiple types:
- Extended-spectrum beta-lactamases (ESBLs): Can hydrolyze extended-spectrum cephalosporins
- Carbapenemases: Can degrade virtually all beta-lactams, including carbapenems
- AmpC beta-lactamases: Typically chromosomally encoded enzymes that can be inducible or derepressed
Target Modification
Bacteria can alter the structure of antibiotic targets while preserving their essential functions.
Altered Penicillin-Binding Proteins (PBPs)
- Methicillin-resistant Staphylococcus aureus (MRSA) produces an alternative PBP (PBP2a) with low affinity for beta-lactams
- This allows cell wall synthesis to continue even in the presence of the antibiotic
Ribosomal Modifications
- Mutations in the 23S rRNA component of the 50S ribosomal subunit confer resistance to macrolides
- Enzymatic methylation of 16S rRNA prevents aminoglycoside binding
- Alterations in ribosomal proteins can disrupt antibiotic binding sites while preserving ribosomal function
DNA Gyrase and Topoisomerase IV Mutations
- Changes in the quinolone resistance-determining regions (QRDRs) of DNA gyrase and topoisomerase IV genes
- These mutations decrease the binding affinity of fluoroquinolones to their target enzymes
Reduced Permeability and Efflux
Bacteria can limit antibiotic accumulation by reducing uptake or actively pumping drugs out of the cell.
Porin Modifications
- Gram-negative bacteria can downregulate or modify outer membrane porins
- This limits the entry of hydrophilic antibiotics like beta-lactams and tetracyclines
- For example, imipenem resistance in Pseudomonas aeruginosa often involves loss of the OprD porin
Efflux Pumps
- Active transport systems that extrude antibiotics from the cell
- Can be specific for certain antibiotics or have broad substrate specificity (multidrug efflux pumps)
- Major families include:
- Resistance-Nodulation-Division (RND) superfamily: Important in gram-negative bacteria
- Major Facilitator Superfamily (MFS): Found in both gram-positive and gram-negative bacteria
- ATP-Binding Cassette (ABC) transporters: Use ATP hydrolysis to drive antibiotic export
- Small Multidrug Resistance (SMR) family: Small proteins that use proton motive force
- Multidrug And Toxic compound Extrusion (MATE) family: Use sodium ion gradients
Bypass of Metabolic Pathways
Bacteria can develop alternative metabolic pathways to circumvent antibiotic-inhibited processes.
Sulfonamide Resistance
- Production of altered dihydropteroate synthase with reduced affinity for sulfonamides
- Increased production of PABA, outcompeting sulfonamides for the enzyme
- Acquisition of alternative folate synthesis pathways
Trimethoprim Resistance
- Production of altered dihydrofolate reductase with reduced drug affinity
- Overexpression of the enzyme to overcome inhibition
- Acquisition of plasmid-encoded resistant dihydrofolate reductase variants
Biofilm Formation
Biofilms represent a complex resistance mechanism involving communities of bacteria.
- Bacteria embed themselves in a self-produced extracellular polymeric substance (EPS)
- The EPS matrix acts as a diffusion barrier, limiting antibiotic penetration
- Reduced metabolic activity of bacteria within biofilms makes them less susceptible to antibiotics that target active processes
- The presence of “persister” cells—dormant variants that survive antibiotic treatment
- Enhanced horizontal gene transfer within biofilms facilitates the spread of resistance genes
4. Genetic Basis of Antibiotic Resistance
Resistance can arise through spontaneous mutations or horizontal gene transfer. Understanding these genetic mechanisms is crucial for tracking resistance spread.
Chromosomal Mutations
Spontaneous mutations in bacterial chromosomes can confer resistance:
- Point mutations: Single nucleotide changes that alter drug targets (e.g., rpoB mutations conferring rifampin resistance)
- Deletions or insertions: Can affect regulatory regions, leading to overexpression of intrinsic resistance mechanisms
- Gene amplification: Multiple copies of resistance genes increase protein expression levels
The mutation rate in bacteria is relatively low (approximately 10⁻¹⁰ per base pair per replication), but large bacterial populations and selective pressure from antibiotics facilitate the emergence of resistant mutants.
Horizontal Gene Transfer
Bacteria can acquire resistance genes from other bacteria through several mechanisms:
Conjugation
- Direct cell-to-cell transfer of genetic material
- Typically involves plasmids carrying resistance genes
- Can transfer large genetic elements encoding multiple resistance determinants
- F plasmids and resistance (R) plasmids are common vectors
Transformation
- Uptake of naked DNA from the environment
- Naturally competent species like Streptococcus pneumoniae can readily acquire resistance genes this way
- The DNA can integrate into the chromosome or exist as a plasmid
Transduction
- Transfer of bacterial DNA via bacteriophages
- Limited by the DNA packaging capacity of the phage
- Important for resistance transfer in some pathogens like Staphylococcus aureus
Mobile Genetic Elements
Several types of mobile genetic elements facilitate resistance gene mobility:
Plasmids
- Self-replicating, extrachromosomal DNA molecules
- Can carry multiple resistance genes and transfer between bacteria
- Conjugative plasmids encode their own transfer apparatus
- Can persist in bacterial populations even without antibiotic pressure due to co-selection or compensatory adaptations
Transposons
- “Jumping genes” that can move between DNA molecules
- Often carry resistance genes
- Simple transposons (Tn3-like) carry single resistance determinants
- Composite transposons (flanked by insertion sequences) can mobilize multiple genes
Integrons
- Genetic capture and expression systems
- Contain an integrase gene, a recombination site, and a promoter
- Capture gene cassettes (often resistance genes) and express them
- Class 1 integrons are particularly important in clinical resistance
Genomic Islands
- Larger chromosomal segments (>10 kb) often containing multiple resistance genes
- Can transfer en bloc between bacteria
- May carry virulence factors alongside resistance determinants
5. Evolution and Spread of Resistance
The emergence and dissemination of antibiotic resistance follows evolutionary principles but is accelerated by human activities.
Selection Pressure
Antibiotic use creates strong selective pressure for resistant bacteria:
- Susceptible bacteria are killed or inhibited, while resistant variants survive
- Even low antibiotic concentrations can select for resistance
- Sub-inhibitory concentrations may promote mutagenesis and horizontal gene transfer
- The “mutant selection window” represents a concentration range where resistant mutants are selectively amplified
Co-selection and Cross-resistance
Resistance mechanisms can be selected by factors beyond the specific antibiotic:
- Co-resistance: Different resistance genes linked on the same genetic element
- Cross-resistance: A single mechanism providing resistance to multiple antibiotics
- Collateral sensitivity: Resistance to one antibiotic increasing susceptibility to another
- Biocide resistance: Selection by disinfectants, antiseptics, or heavy metals can co-select for antibiotic resistance
Fitness Costs and Compensation
Resistance often imposes metabolic burdens on bacteria:
- Initial resistance mutations may reduce bacterial fitness in antibiotic-free environments
- Compensatory mutations can ameliorate these fitness costs
- Low-fitness cost resistance is more likely to persist even without antibiotic pressure
- Some resistance mechanisms may actually confer a fitness advantage in certain environments
Transmission Dynamics
Understanding how resistant bacteria spread is essential for control strategies:
- Healthcare settings: Close patient proximity, vulnerable hosts, and high antibiotic use create ideal conditions for resistance spread
- Community transmission: Increasing problem with community-acquired MRSA and ESBLs
- Environmental reservoirs: Soil, water, and wildlife can harbor resistance genes
- Food production: Agricultural antibiotic use selects for resistant bacteria that can transfer to humans
- Global travel: Rapid movement of people and goods facilitates worldwide dissemination of resistant clones
6. Clinical Impact and Management
Antibiotic resistance has profound implications for patient care and healthcare systems.
Treatment Failures
Resistant infections lead to:
- Prolonged illness duration
- Increased mortality rates
- Need for more toxic or expensive second-line agents
- Extended hospital stays
- Higher healthcare costs
Surveillance Systems
Monitoring resistance trends guides clinical and policy decisions:
- Local hospital antibiograms: Guide empiric therapy choices
- National surveillance networks: Track emerging threats
- Global initiatives: World Health Organization’s Global Antimicrobial Resistance Surveillance System (GLASS)
- Molecular surveillance: Whole genome sequencing to track resistant clones
Antibiotic Stewardship
Coordinated programs to improve appropriate antibiotic use:
- Evidence-based prescribing guidelines
- Restriction of broad-spectrum agents
- Prospective audit and feedback
- Education for healthcare providers and patients
- Rapid diagnostic testing to guide therapy
- Optimized dosing and duration
Infection Prevention and Control
Preventing transmission reduces the burden of resistant infections:
- Standard and transmission-based precautions
- Hand hygiene compliance
- Environmental cleaning and disinfection
- Active surveillance for resistant organisms
- Patient isolation and cohorting
- Decolonization strategies for carriers
7. New Approaches to Combat Resistance
The arms race between antibiotics and resistance requires innovative countermeasures.
Novel Antibiotic Development
New drugs targeting unexploited bacterial vulnerabilities:
- Teixobactin: Inhibits cell wall synthesis through a novel mechanism
- Arylomycins: Target bacterial signal peptidase
- Gepotidacin: Inhibits DNA gyrase at a site distinct from fluoroquinolones
- Murepavadin: Targets the outer membrane protein LptD in Pseudomonas
Combination Therapies
Strategic antibiotic combinations can overcome resistance:
- Beta-lactam/beta-lactamase inhibitor combinations (e.g., ceftazidime-avibactam)
- Dual-action antibiotics (e.g., cefiderocol, which combines siderophore and beta-lactam activities)
- Antibiotic adjuvants that don’t have antibacterial activity but enhance effectiveness
Alternative Approaches
Non-antibiotic strategies to combat bacterial infections:
- Bacteriophage therapy: Viruses that specifically infect and kill bacteria
- Antimicrobial peptides: Natural or synthetic peptides with direct antibacterial activity
- Anti-virulence compounds: Target bacterial virulence rather than growth
- Microbiome manipulation: Probiotics or fecal microbiota transplantation
- Immune modulation: Enhance host defense mechanisms
- CRISPR-Cas systems: Targeted bacterial DNA cleavage
8. Frequently Asked Questions (FAQ)
Q1: Why do antibiotics work against bacteria but not viruses? A: Antibiotics target structures or processes that are specific to bacterial cells, such as the peptidoglycan cell wall, 70S ribosomes, or bacterial enzymes. Viruses lack these structures and rely on host cell machinery for replication, making them unaffected by antibiotics. Viral infections require antiviral medications that target virus-specific processes.
Q2: What is the difference between bactericidal and bacteriostatic antibiotics? A: Bactericidal antibiotics kill bacteria directly by causing cell death, while bacteriostatic antibiotics inhibit bacterial growth without necessarily killing them. Bactericidal drugs include beta-lactams, aminoglycosides, and fluoroquinolones, while bacteriostatic drugs include tetracyclines, macrolides, and sulfonamides. The distinction can be concentration-dependent, with some antibiotics being bacteriostatic at low concentrations and bactericidal at higher doses.
Q3: How quickly can bacteria develop resistance to new antibiotics? A: Resistance can emerge rapidly, sometimes within months of a new antibiotic’s introduction into clinical practice. The timeframe depends on multiple factors including the antibiotic’s mechanism, the prevalence of pre-existing resistance mechanisms, the mutation rate of the target bacteria, and the intensity of selective pressure. Resistance to daptomycin was reported within a year of its approval, while resistance to linezolid emerged within a few years.
Q4: Can antibiotic resistance be reversed? A: In some cases, yes. When antibiotic pressure is removed, resistant bacteria may be outcompeted by susceptible strains if the resistance mechanism imposes a fitness cost. However, compensatory mutations often reduce these fitness costs, allowing resistance to persist. Some countries have successfully reduced resistance rates through antibiotic stewardship and infection control measures, but complete reversal is rare once resistance becomes established in a population.
Q5: Do probiotics help prevent antibiotic resistance? A: Probiotics don’t directly prevent the development of resistance mutations or gene transfer in pathogens. However, they may help maintain a healthy microbiome during antibiotic treatment, potentially reducing the risk of colonization by resistant organisms. Some probiotics may also compete with pathogens for resources and produce antimicrobial compounds. Research in this area is ongoing, but probiotics should be considered a complement to, not a replacement for, appropriate antibiotic use.
Q6: What is the “post-antibiotic era” that experts warn about? A: The “post-antibiotic era” refers to a potential future where common bacterial infections once again become untreatable due to widespread antibiotic resistance. In such a scenario, routine medical procedures that rely on effective antibiotics (like surgeries, cancer chemotherapy, and organ transplantation) would become significantly more dangerous. While we haven’t reached this point globally, some highly resistant infections already have extremely limited treatment options, representing a concerning preview of this possible future.
Q7: Do antibiotics cause resistance or just select for it? A: Both processes occur. Antibiotics primarily select for pre-existing resistant variants by eliminating susceptible bacteria. However, some antibiotics can also increase mutation rates or stimulate horizontal gene transfer through the bacterial SOS response, actively promoting the development of new resistance. Additionally, sub-inhibitory antibiotic concentrations can induce specific resistance mechanisms and create selective environments that favor resistance evolution.
Q8: Are natural antibiotics less likely to generate resistance than synthetic ones? A: No. Resistance can develop against both natural and synthetic antibiotics. In fact, resistance mechanisms against natural antibiotics have existed in environmental bacteria for millions of years, as these compounds are part of the natural competitive dynamics between microorganisms. Synthetic antibiotics may initially encounter less pre-existing resistance, but bacteria can still evolve new mechanisms against them. The chemical structure and mechanism of action, rather than natural versus synthetic origin, are more relevant factors in resistance development.
References
- Blair JMA, Webber MA, Baylay AJ, et al. Molecular mechanisms of antibiotic resistance. Nature Reviews Microbiology. 2015;13(1):42-51. https://www.nature.com/articles/nrmicro3380
- World Health Organization. Global action plan on antimicrobial resistance. 2015. https://www.who.int/publications/i/item/9789241509763
- Kapoor G, Saigal S, Elongavan A. Action and resistance mechanisms of antibiotics: A guide for clinicians. Journal of Anaesthesiology Clinical Pharmacology. 2017;33(3):300-305. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5672523/
- Holmes AH, Moore LS, Sundsfjord A, et al. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet. 2016;387(10014):176-187. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(15)00473-0/fulltext
- Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2019. Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2019. https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf
- Munita JM, Arias CA. Mechanisms of antibiotic resistance. Microbiology Spectrum. 2016;4(2). https://journals.asm.org/doi/10.1128/microbiolspec.VMBF-0016-2015
- Li XZ, Plésiat P, Nikaido H. The challenge of efflux-mediated antibiotic resistance in Gram-negative bacteria. Clinical Microbiology Reviews. 2015;28(2):337-418. https://journals.asm.org/doi/10.1128/CMR.00117-14
- Baquero F, Coque TM, de la Cruz F. Ecology and evolution as targets: the need for novel eco-evo drugs and strategies to fight antibiotic resistance. Antimicrobial Agents and Chemotherapy. 2011;55(8):3649-3660. https://journals.asm.org/doi/10.1128/AAC.00013-11
- Walsh C. Molecular mechanisms that confer antibacterial drug resistance. Nature. 2000;406(6797):775-781. https://www.nature.com/articles/35021219
- Theuretzbacher U, Bush K, Harbarth S, et al. Critical analysis of antibacterial agents in clinical development. Nature Reviews Microbiology. 2020;18(5):286-298. https://www.nature.com/articles/s41579-020-0340-0