What is Plasmodium falciparum?
Plasmodium falciparum is a protozoan parasite that causes the most severe form of malaria in humans. It is transmitted through the bite of an infected female Anopheles mosquito. P. falciparum is responsible for the majority of malaria-related morbidity and mortality worldwide, particularly in tropical and subtropical regions.
Biology and Characteristics of Plasmodium falciparum
Morphology
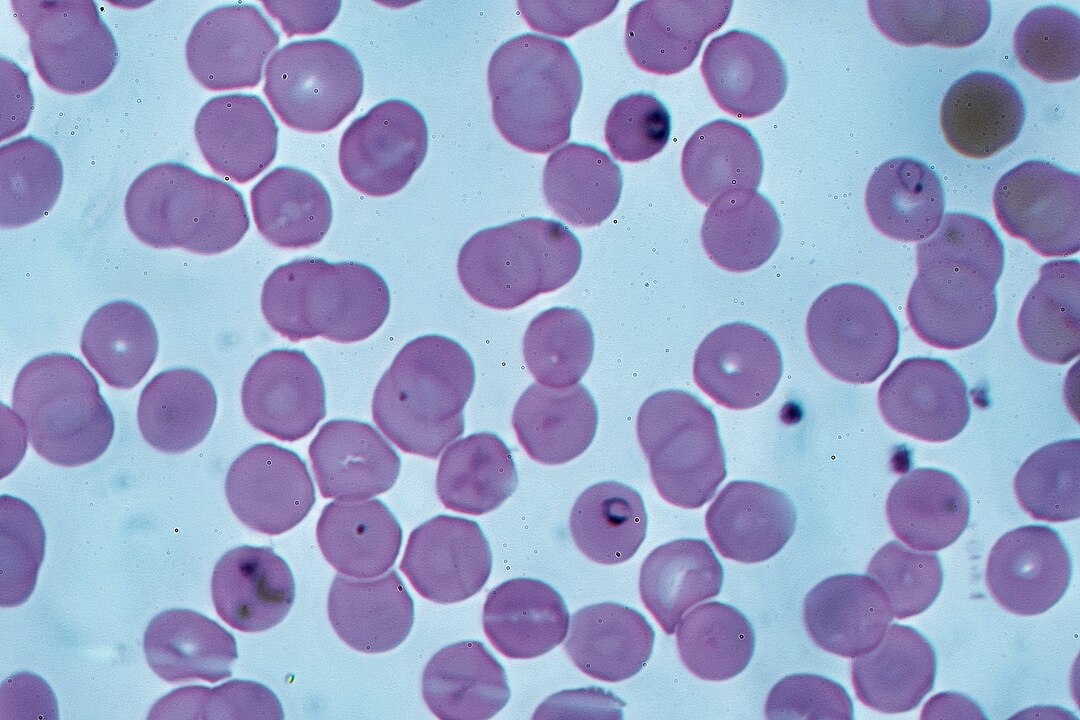
- Shape: Irregular, amoeboid shape in the erythrocytic stage.
- Size: Approximately 1.5-2 µm in diameter.
- Staining: Appears as ring forms, trophozoites, schizonts, and gametocytes in Giemsa-stained blood smears.
Habitat
- Human Host: Resides in the liver and red blood cells during its life cycle.
- Mosquito Host: Completes sexual reproduction in the gut of the Anopheles mosquito.
Genetic Diversity
- P. falciparum exhibits high genetic variability, contributing to its ability to evade the immune system and develop drug resistance.
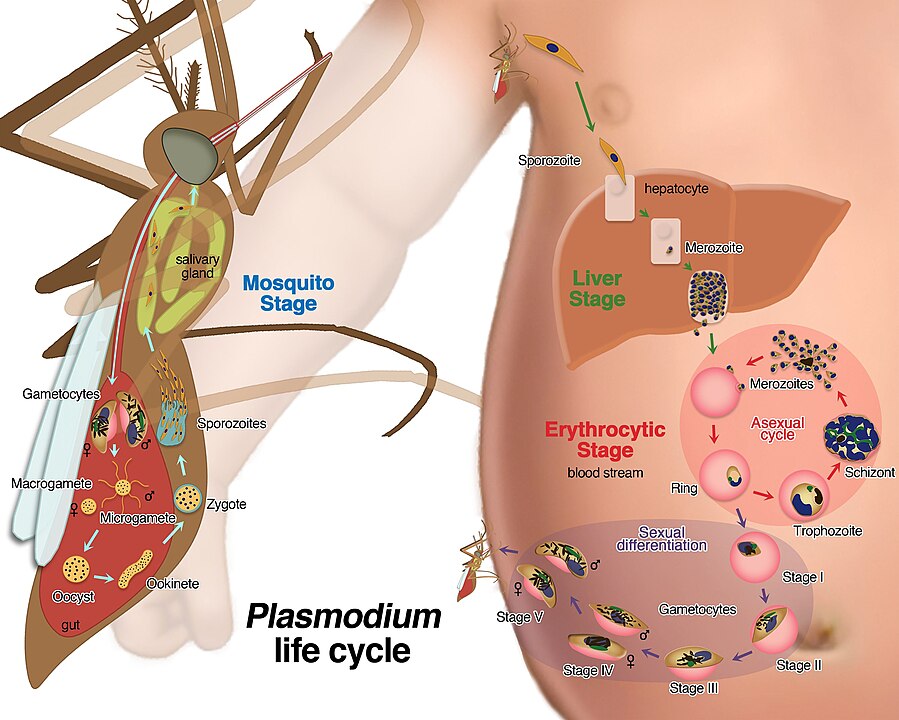
Life Cycle of Plasmodium falciparum
Transmission
- The life cycle begins when an infected female Anopheles mosquito bites a human, injecting sporozoites into the bloodstream.
Liver Stage (Exo-erythrocytic Stage)
- Sporozoites: Travel to the liver and invade hepatocytes.
- Schizogony: Multiply asexually to form thousands of merozoites.
- Release: Merozoites are released into the bloodstream, initiating the erythrocytic stage.
Blood Stage (Erythrocytic Stage)
- Merozoites: Invade red blood cells (RBCs) and develop into trophozoites.
- Ring Stage: Early trophozoites appear as ring forms in blood smears.
- Schizonts: Mature trophozoites undergo schizogony, producing more merozoites.
- Rupture: Infected RBCs rupture, releasing merozoites to infect new RBCs.
Sexual Stage (Gametocytogenesis)
- Gametocytes: Some merozoites develop into male (microgametocytes) and female (macrogametocytes) gametocytes.
- Mosquito Ingestion: Gametocytes are taken up by a mosquito during a blood meal.
Mosquito Stage (Sporogony)
- Fertilization: Gametocytes fuse to form zygotes in the mosquito’s gut.
- Oocysts: Zygotes develop into oocysts, which release sporozoites.
- Migration: Sporozoites migrate to the mosquito’s salivary glands, ready to infect a new host.
Symptoms of Falciparum Malaria
Incubation Period
- Typically ranges from 7 to 14 days after the infective mosquito bite.
Clinical Manifestations
- Fever: High fever with chills and sweating, often cyclical.
- Headache: Severe headaches are common.
- Fatigue: Extreme tiredness and malaise.
- Nausea and Vomiting: Gastrointestinal symptoms are frequent.
- Anemia: Due to the destruction of red blood cells.
- Jaundice: Resulting from hemolysis and liver dysfunction.
Severe Malaria Complications
- Cerebral Malaria: Altered mental status, seizures, and coma due to brain involvement.
- Severe Anemia: Life-threatening reduction in red blood cells.
- Acute Respiratory Distress Syndrome (ARDS): Difficulty breathing due to lung involvement.
- Renal Failure: Impaired kidney function.
- Hypoglycemia: Low blood sugar, particularly in pregnant women and children.
Diagnosis of Plasmodium falciparum Infection
Microscopic Examination
- Thick and Thin Blood Smears: Gold standard for diagnosis.
- Thick Smear: Detects the presence of parasites.
- Thin Smear: Identifies the species and stage of the parasite.
Rapid Diagnostic Tests (RDTs)
- Detects specific antigens (e.g., HRP-2) produced by P. falciparum.
- Provides quick results but less sensitive than microscopy.
Molecular Diagnostics
- Polymerase Chain Reaction (PCR): Highly sensitive and specific for detecting P. falciparum DNA.
- Useful for confirming diagnosis and detecting drug resistance.
Serology
- Detects antibodies against P. falciparum, indicating past infection.
- Not useful for acute diagnosis.
Treatment of Falciparum Malaria
Antimalarial Drugs
- Artemisinin-based Combination Therapies (ACTs): First-line treatment for uncomplicated falciparum malaria.
- Examples: Artemether-lumefantrine, artesunate-amodiaquine.
- Quinine: Used for severe malaria, often in combination with doxycycline or clindamycin.
- Mefloquine: Alternative for uncomplicated malaria in areas with chloroquine resistance.
Severe Malaria Treatment
- Intravenous Artesunate: Preferred for severe malaria.
- Intravenous Quinine: Alternative if artesunate is unavailable.
- Supportive Care: Includes management of complications such as seizures, anemia, and renal failure.
Drug Resistance
- P. falciparum has developed resistance to several antimalarial drugs, including chloroquine and sulfadoxine-pyrimethamine.
- Continuous monitoring and development of new drugs are essential.
Prevention and Control of Malaria
Vector Control
- Insecticide-Treated Nets (ITNs): Reduce mosquito bites during sleep.
- Indoor Residual Spraying (IRS): Application of insecticides to indoor surfaces to kill mosquitoes.
Chemoprophylaxis
- Antimalarial Drugs: Taken by travelers to malaria-endemic areas.
- Examples: Atovaquone-proguanil, doxycycline, mefloquine.
Vaccination
- RTS,S/AS01 (Mosquirix): The first malaria vaccine approved for use in children in endemic areas.
- Provides partial protection and is used in combination with other preventive measures.
Environmental Management
- Reducing mosquito breeding sites by eliminating standing water.
- Promoting community awareness and education.
Global Impact of Plasmodium falciparum
Epidemiology
- P. falciparum is prevalent in sub-Saharan Africa, Southeast Asia, and parts of South America.
- Accounts for approximately 99% of malaria deaths globally.
Mortality Rate
- In 2020, there were an estimated 627,000 malaria deaths, with children under five being the most vulnerable.
Economic Burden
- Malaria imposes a significant economic burden on affected countries, reducing productivity and increasing healthcare costs.
Efforts to Eliminate Malaria
- The World Health Organization (WHO) aims to reduce malaria incidence and mortality by 90% by 2030.
- Strategies include scaling up prevention, improving diagnostic and treatment access, and developing new tools.
Frequently Asked Questions (FAQs)
Q1: Can malaria be transmitted through blood transfusion?
- Yes, malaria can be transmitted through infected blood transfusions or organ transplants.
Q2: Is there a vaccine for Plasmodium falciparum?
- Yes, the RTS,S/AS01 vaccine provides partial protection and is recommended for children in endemic areas.
Q3: How can I prevent malaria while traveling?
- Use insect repellent, sleep under insecticide-treated nets, and take antimalarial prophylaxis as prescribed.
Q4: Can malaria recur after treatment?
- Yes, P. falciparum can cause relapses if not treated properly. Follow-up and adherence to treatment are crucial.
References
- World Health Organization (WHO). Malaria. Link
- Centers for Disease Control and Prevention (CDC). Malaria Diagnosis & Treatment. Link
- Mayo Clinic. Malaria Symptoms and Causes. Link
- National Institute of Allergy and Infectious Diseases (NIAID). Malaria. Link
SEO Keywords: Plasmodium falciparum, malaria symptoms, malaria treatment, malaria prevention, falciparum malaria, malaria parasite, malaria diagnosis, malaria life cycle, malaria vaccine, malaria complications.