Introduction
Mycobacterium leprae is the primary causative agent of leprosy (also known as Hansen’s disease), a chronic infectious disease with a long and complex history in human civilization. This article provides a comprehensive overview of this unique bacterium, its characteristics, the disease it causes, diagnosis, treatment approaches, and the current global situation regarding leprosy.
Biological Characteristics of Mycobacterium leprae
Taxonomic Classification
M. leprae belongs to the family Mycobacteriaceae, genus Mycobacterium. It is related to other medically significant mycobacteria such as M. tuberculosis (which causes tuberculosis) and M. avium complex.
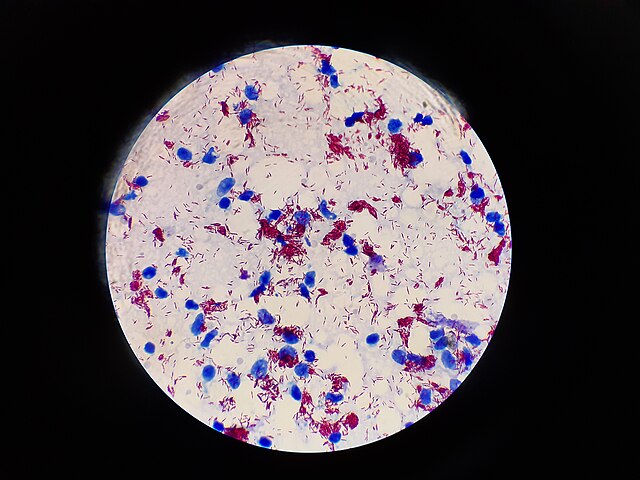
Morphology and Staining Properties
- Cell Shape and Size: Rod-shaped (bacillus) with dimensions of approximately 1-8 μm in length and 0.2-0.5 μm in width
- Cell Wall Structure: Exceptionally thick cell wall rich in mycolic acids, which provides:
- Resistance to environmental stresses
- Acid-fast staining properties (retains certain dyes even after acid washing)
- Protection against many antimicrobial agents
- Staining Characteristics: Acid-fast positive using Ziehl-Neelsen or Fite-Faraco staining methods
Growth Characteristics
M. leprae has several unique growth properties that make it exceptionally challenging to study:
| Characteristic | Description |
|---|---|
| In vitro cultivation | Cannot be cultured on artificial media in laboratories |
| Generation time | Extremely slow (12-14 days) – the slowest growing human pathogen |
| Growth temperature | Optimal growth at cooler temperatures (30-33°C) rather than normal body temperature (37°C) |
| Preferred sites | Grows best in cooler body regions: skin, peripheral nerves, upper respiratory tract, testes, anterior chamber of the eye |
| Host range | Primarily infects humans and nine-banded armadillos; can also grow in mouse footpads and certain primates |
Genomic Features
The genome of M. leprae was completely sequenced in 2001, revealing several fascinating characteristics:
| Genomic Feature | Details |
|---|---|
| Genome size | 3.27 million base pairs (significantly smaller than M. tuberculosis) |
| Pseudogenes | Contains over 1,100 pseudogenes (non-functional genes) |
| Functional genes | Only about 1,600 functional genes (compared to 4,000 in M. tuberculosis) |
| Genome reduction | Evidence of massive genome reduction/decay over evolutionary time |
| Metabolic capacity | Extremely limited metabolic capabilities due to gene loss |
The extensive genome degradation explains why M. leprae is an obligate intracellular pathogen that cannot be cultured outside living cells – it has lost the genes necessary for independent survival.

Transmission and Pathogenesis
Transmission Routes
- Primary Route: Respiratory droplets from untreated multibacillary leprosy patients
- Secondary Routes:
- Prolonged direct skin contact with skin lesions
- Possible transmission via insect vectors (though evidence is limited)
- Environmental reservoirs (armadillos in the southern United States)
- Important Note: Despite common misconceptions, leprosy is not highly contagious – approximately 95% of humans have natural immunity to the infection
Disease Development
| Stage | Process |
|---|---|
| Entry | Bacteria enter through respiratory tract or broken skin |
| Initial infection | Bacteria are taken up by macrophages and Schwann cells |
| Incubation | Extremely long incubation period (3-5 years average, can be up to 20 years) |
| Bacterial multiplication | Slow replication within cells, especially Schwann cells surrounding peripheral nerves |
| Disease manifestation | Clinical presentation depends on host immune response |
Immunological Response
The clinical manifestations of leprosy exist on a spectrum determined by the host’s immune response:
| Leprosy Type | Immune Response | Bacterial Load | Clinical Features |
|---|---|---|---|
| Tuberculoid (paucibacillary) | Strong cell-mediated (Th1) immune response | Low (few bacteria) | Few well-defined lesions, significant nerve damage |
| Lepromatous (multibacillary) | Poor cell-mediated immunity, strong humoral (Th2) response | High (many bacteria) | Widespread lesions, nodules, diffuse infiltration |
| Borderline forms | Intermediate immune responses | Variable | Mixed features |
Pathological Effects
M. leprae primarily affects:
- Peripheral nerves: Has unique tropism for Schwann cells, leading to demyelination and nerve damage
- Skin: Causes various dermatological manifestations
- Upper respiratory tract mucosa: Particularly the nasal mucosa
- Eyes: Can cause various ocular complications
- Testes: May cause orchitis and hypogonadism in males
Clinical Manifestations of Leprosy
Cardinal Signs
- Hypopigmented or reddish skin patches with reduced sensation
- Thickened peripheral nerves with associated sensory/motor deficits
- Acid-fast bacilli in skin smears or biopsies
Classification Systems
Two main classification systems are used for leprosy:
Ridley-Jopling Classification
| Type | Characteristics | Bacterial Index |
|---|---|---|
| TT (Tuberculoid) | Few lesions, well-defined, asymmetric, anesthetic | 0 |
| BT (Borderline Tuberculoid) | More numerous lesions than TT | 0-1+ |
| BB (Mid-Borderline) | Intermediate characteristics | 2-3+ |
| BL (Borderline Lepromatous) | Numerous lesions, moderately defined | 4-5+ |
| LL (Lepromatous) | Numerous, poorly defined, symmetric lesions | 5-6+ |
WHO Classification (for Treatment Purposes)
| Type | Definition | Treatment |
|---|---|---|
| Paucibacillary (PB) | 1-5 skin lesions and/or one nerve trunk involvement | 6-month MDT regimen |
| Multibacillary (MB) | >5 skin lesions and/or more than one nerve trunk involvement | 12-month MDT regimen |
Complications
Long-term or untreated leprosy can lead to severe complications:
| Complication | Description |
|---|---|
| Deformities | Claw hand, foot drop, facial deformities due to nerve damage |
| Contractures | Permanent flexion of fingers and toes |
| Absorption of digits | Loss of fingers and toes due to repeated trauma and infection |
| Blindness | Due to corneal damage, iridocyclitis, or lagophthalmos |
| Secondary infections | Due to loss of sensation and protective functions |
| Leprosy reactions | Type 1 (reversal) and Type 2 (ENL) reactions causing acute nerve damage |
Diagnosis
Clinical Diagnosis
- Detailed examination of skin lesions for sensation, color, and distribution
- Assessment of peripheral nerves for enlargement and tenderness
- Evaluation of motor and sensory functions
Laboratory Diagnosis
| Diagnostic Method | Description | Application |
|---|---|---|
| Slit-skin smear | Microscopic examination of skin smears for acid-fast bacilli | Confirms diagnosis, determines bacterial load |
| Skin biopsy | Histopathological examination of skin tissue | Gold standard, confirms diagnosis and type |
| PCR | Detection of M. leprae DNA | Highly sensitive, especially for paucibacillary cases |
| Serological tests | Detection of antibodies (anti-PGL-I) | Used for screening in high-endemic areas |
| Lepromin test | Measures cell-mediated immunity to M. leprae | Used for classification, not diagnosis |
Differential Diagnosis
Various conditions may resemble leprosy:
- Vitiligo
- Tinea versicolor
- Cutaneous leishmaniasis
- Sarcoidosis
- Post-kala-azar dermal leishmaniasis
- Various peripheral neuropathies
Treatment
Multi-Drug Therapy (MDT)
The WHO-recommended treatment involves a combination of antibiotics:
| Leprosy Type | Drug Regimen | Duration |
|---|---|---|
| Paucibacillary | Rifampicin (600 mg once monthly, supervised) + Dapsone (100 mg daily, self-administered) | 6 months |
| Multibacillary | Rifampicin (600 mg once monthly, supervised) + Clofazimine (300 mg once monthly, supervised and 50 mg daily, self-administered) + Dapsone (100 mg daily, self-administered) | 12 months |
Management of Leprosy Reactions
| Reaction Type | Clinical Features | Treatment |
|---|---|---|
| Type 1 (Reversal) | Increased inflammation in existing lesions, new lesions, nerve pain | Corticosteroids (Prednisolone) |
| Type 2 (ENL) | Painful nodules, fever, joint pain, iritis, neuritis | Thalidomide (with strict controls), Clofazimine, Corticosteroids |
Rehabilitation
- Physical therapy to prevent disabilities
- Reconstructive surgery for established deformities
- Protective footwear and adaptive devices
- Psychological support and counseling
- Vocational training and socioeconomic rehabilitation
Epidemiology and Public Health
Global Burden
- According to WHO, approximately 200,000 new cases are reported annually
- Major endemic countries include India, Brazil, and Indonesia
- Global registered prevalence: approximately 0.2 cases per 10,000 population
High-Risk Groups
- Household contacts of untreated multibacillary patients
- Individuals living in endemic regions
- People living in poverty with limited access to healthcare
- Individuals with compromised immune systems
Prevention Strategies
- Early detection and treatment
- Contact tracing and follow-up
- BCG vaccination (provides variable protection)
- Health education and reducing stigma
- Improved living conditions and nutrition
Elimination Strategy
The WHO defined elimination of leprosy as a public health problem as achieving a prevalence of less than 1 case per 10,000 population. While this has been achieved at the global level and in most countries, pockets of high endemicity still exist.
Recent Research and Future Directions
Diagnostics
- Development of rapid point-of-care diagnostic tests
- Improved molecular methods for early detection
- Field-friendly tools for nerve damage assessment
Therapeutics
- New antibiotic combinations to shorten treatment duration
- Development of immunomodulatory agents to prevent reactions
- Targeted therapies to prevent nerve damage
Vaccine Development
- Development of specific vaccines against M. leprae
- Enhancement of BCG vaccine efficacy for leprosy
Genomics and Molecular Biology
- Further understanding of M. leprae’s unique biology
- Identification of drug targets and virulence factors
- Studies on M. leprae’s evolution and host adaptation
Historical and Social Aspects
Historical Significance
- One of the oldest recorded human diseases (dating back to 2000 BCE)
- Mentioned in ancient texts from various civilizations
- Led to significant stigmatization and isolation throughout history
Stigma and Social Impact
- Historical isolation in “leper colonies”
- Religious and cultural interpretations of the disease
- Modern-day discrimination and social exclusion in some regions
- Impact on mental health and quality of life
Notable Figures
- Gerhard Armauer Hansen (identified M. leprae in 1873)
- Father Damien (dedicated his life to leprosy patients in Hawaii)
- Stanley Stein (advocated for destigmatization through “The Star” publication)
- Mother Teresa (worked with leprosy patients in India)
Frequently Asked Questions (FAQ)
Q1. Is leprosy highly contagious?
No, leprosy is not highly contagious. Approximately 95% of people have natural immunity to M. leprae. Transmission typically requires prolonged, close contact with an untreated individual with multibacillary leprosy.
Q2. Can leprosy be cured completely?
Yes, leprosy is completely curable with multi-drug therapy (MDT). Early diagnosis and treatment prevent disability and stop transmission.
Q3. Does leprosy cause body parts to fall off?
No, contrary to popular belief, leprosy does not cause body parts to “fall off.” However, untreated leprosy can lead to nerve damage, resulting in loss of sensation. This loss of sensation can lead to unnoticed injuries, infections, and eventual tissue loss.
Q4. Is there a vaccine for leprosy?
There is no specific vaccine for leprosy, but the BCG vaccine (primarily used against tuberculosis) provides some protection against leprosy, with effectiveness varying from 20-80% depending on the study.
Q5. Can someone with leprosy live a normal life?
Yes, with early diagnosis and proper treatment, people with leprosy can live completely normal lives without disability. Even those with some disability can lead productive lives with proper support and rehabilitation.
Q6. Are there drug-resistant strains of M. leprae?
Yes, there have been reports of M. leprae strains resistant to one or more of the drugs used in MDT. This is one reason why combination therapy is important.
Q7. How long does leprosy treatment take?
Treatment duration depends on the type of leprosy: 6 months for paucibacillary cases and 12 months for multibacillary cases using WHO-recommended MDT regimens.
Q8. Can leprosy recur after treatment?
True relapse of leprosy after complete MDT is relatively rare (less than 1% of cases). However, leprosy reactions can occur even after completing treatment and should not be confused with relapse.
Q9. Can leprosy be transmitted from mother to child during pregnancy?
Transplacental transmission of M. leprae is rare but possible. Children born to mothers with untreated leprosy should be monitored closely.
Q10. Are animals a significant source of leprosy infection?
In most parts of the world, humans are the main reservoir of M. leprae. However, in the southern United States, wild armadillos can carry M. leprae and have been linked to some human cases.
References
- World Health Organization. (2023). “Global Leprosy (Hansen’s Disease) Update, 2022: Moving towards Elimination.” Weekly Epidemiological Record. https://www.who.int/publications/i/item/who-wer-9836-424-440
- Scollard, D.M., Adams, L.B., Gillis, T.P., Krahenbuhl, J.L., Truman, R.W., & Williams, D.L. (2006). “The Continuing Challenges of Leprosy.” Clinical Microbiology Reviews, 19(2), 338-381. https://cmr.asm.org/content/19/2/338
- Cole, S.T., Eiglmeier, K., Parkhill, J., James, K.D., Thomson, N.R., Wheeler, P.R., et al. (2001). “Massive gene decay in the leprosy bacillus.” Nature, 409(6823), 1007-1011. https://www.nature.com/articles/35059006
- Britton, W.J., & Lockwood, D.N. (2004). “Leprosy.” The Lancet, 363(9416), 1209-1219. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(04)15952-7/fulltext
- International Leprosy Association. (2024). “Technical Resources.” https://leprosyassociation.org/resources/technical-resources
- National Hansen’s Disease (Leprosy) Program. (2024). “Guide to the Diagnosis and Treatment of Hansen’s Disease.” Health Resources and Services Administration, U.S. Department of Health and Human Services. https://www.hrsa.gov/hansens-disease/diagnosis
- Rodrigues, L.C., & Lockwood, D.N. (2011). “Leprosy now: epidemiology, progress, challenges, and research gaps.” The Lancet Infectious Diseases, 11(6), 464-470. https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(11)70006-8/fulltext
- Singh, P., & Cole, S.T. (2011). “Mycobacterium leprae: genes, pseudogenes and genetic diversity.” Future Microbiology, 6(1), 57-71. https://www.futuremedicine.com/doi/10.2217/fmb.10.153
- Walker, S.L., & Lockwood, D.N. (2006). “The clinical and immunological features of leprosy.” British Medical Bulletin, 77-78, 103-121. https://academic.oup.com/bmb/article/77-78/1/103/313209
- Truman, R.W., Singh, P., Sharma, R., Busso, P., Rougemont, J., Paniz-Mondolfi, A., et al. (2011). “Probable zoonotic leprosy in the southern United States.” New England Journal of Medicine, 364(17), 1626-1633. https://www.nejm.org/doi/full/10.1056/NEJMoa1010536